


What Is Alveolitis? Dry Socket Treatment After Tooth Extraction
Don't put off your smile. Message us now to discuss your treatment options with our expert dentists.
WhatsAppIn clinical dentistry, tooth extraction remains a routine surgical procedure that becomes inevitable in the presence of extensive decay, vertical root fractures, severe bone loss, or impacted third molars, even though conservative therapies are always prioritized. Most patients return to their daily routines without any issues following several hours of post-operative numbness under successful local anesthesia. However, sometimes, no matter how flawlessly the procedure is performed, the biological healing window does not progress as planned.
Following an initial 24-to-48-hour period of mild post-operative soreness, a sudden, intense, throbbing pain can develop, spreading toward the ear and temple and completely resisting standard painkillers. Defined in medical literature as alveolitis (alveolar osteitis) or commonly known as dry socket, this condition represents one of the most painful restorative complications encountered after a tooth extraction. When not intervened in time, it leaves the patient dealing with sleepless nights. However, thanks to contemporary oral surgery protocols, it can be fully controlled with a short 10-minute dressing appointment. In this comprehensive expert guide, we examine the causes, structural appearance, and modern clinical treatments of alveolitis in full detail.
Table of Content
- What is Alveolitis After Tooth Extraction and Why Does It Occur?
- What Causes Alveolitis? What Are the Primary Risk Factors?
- What Are the Symptoms of Alveolitis and How is it Detected?
- How Does Alveolitis Look? Structural Appearance
- How is Contemporary Alveolitis Treatment Done and How Does It Heal?
- Frequently Asked Questions
What is Alveolitis After Tooth Extraction and Why Does It Occur?
Based on the most accurate medical definition from clinical follow-ups, alveolitis after tooth extraction is a condition where the biological healing mechanism of the extraction socket (alveolar bone) is disrupted.
But what exactly is the underlying pathology of what is alveolitis and why does it occur systemically?
Immediately following a normal tooth extraction, blood fills the empty socket, and within seconds, a red, gel-like protective blood clot (coagulum) forms. This clot acts as a natural "biological barrier" that shields the bare walls of the jawbone and the deep, open nerve endings from oral bacteria, food acids, and thermal external factors (hot and cold). Over time, this blood clot organizes and transforms into new bone and gum tissue.
However, if this blood clot never forms due to certain triggering factors, or if it disintegrates and is dislodged prematurely from the socket within the first few days, the jawbone is left entirely defenseless and exposed. The direct contact of the bone walls with air and bacteria initiates inflammation, leading to the development of alveolitis.
What Causes Alveolitis? What Are the Primary Risk Factors?

The primary elements that sabotage the delicate clot mechanism within the extraction socket and trigger the development of alveolitis include:
- Smoking and Tobacco Use: Nicotine in tobacco smoke constricts blood vessels, reducing vital blood flow to the extraction site. Most dangerously, the suction motion performed while smoking or vaping creates negative pressure inside the oral cavity, pulling the freshly formed blood clot out of its socket like a vacuum.
- Poor Oral Hygiene, Spitting, and Straw Use: Aggressive spitting, rinsing the mouth with water, or consuming beverages through a straw during the first day post-extraction are the leading causes of premature clot disruption.
- Birth Control Pills (Estrogen Hormone): In female patients with high estrogen levels or those taking oral contraceptives, the hormone levels accelerate the body's fibrinolysis (clot-dissolving) mechanism, shortening the lifespan of the protective blood clot.
- Difficult and Traumatic Extractions: Especially in surgical extractions of horizontally impacted wisdom teeth that require bone removal, prolonged surgery times and structural trauma to the bone matrix elevate the risk of alveolitis to the 20-30% range.
What Are the Symptoms of Alveolitis and How is it Detected?
A patient's ability to differentiate between normal post-extraction soreness and acute alveolitis pain is critical for timely treatment. The clinical signs of how alveolitis is recognized and the most prominent alveolitis symptoms include:
- Delayed Onset of Severe Pain: While everything appears normal during the first two days following extraction, a sudden, throbbing, and progressively worsening pain begins on the 3rd to 5th day.
- Radiating Pain Architecture: The pain does not remain localized to the extraction site; it radiates across a broad area, spreading toward the ear, temple, under the eye, the entire lower jawbone, and the neck.
- Bad Breath and Foul Taste: Food debris gathering inside the socket where the blood clot was lost begins to decay rapidly in an anaerobic environment. This creates a distinct foul odor (halitosis) resembling rotten eggs and a bitter, metallic taste in the patient's mouth.
- Mild Lymph Node Swelling: Tenderness and slight swelling of the lymph nodes under the jaw and along the neck may accompany the condition. However, systemic high fever or severe facial swelling are generally absent in typical alveolitis; if these symptoms present, the clinical scenario points to an odontogenic abscess instead.
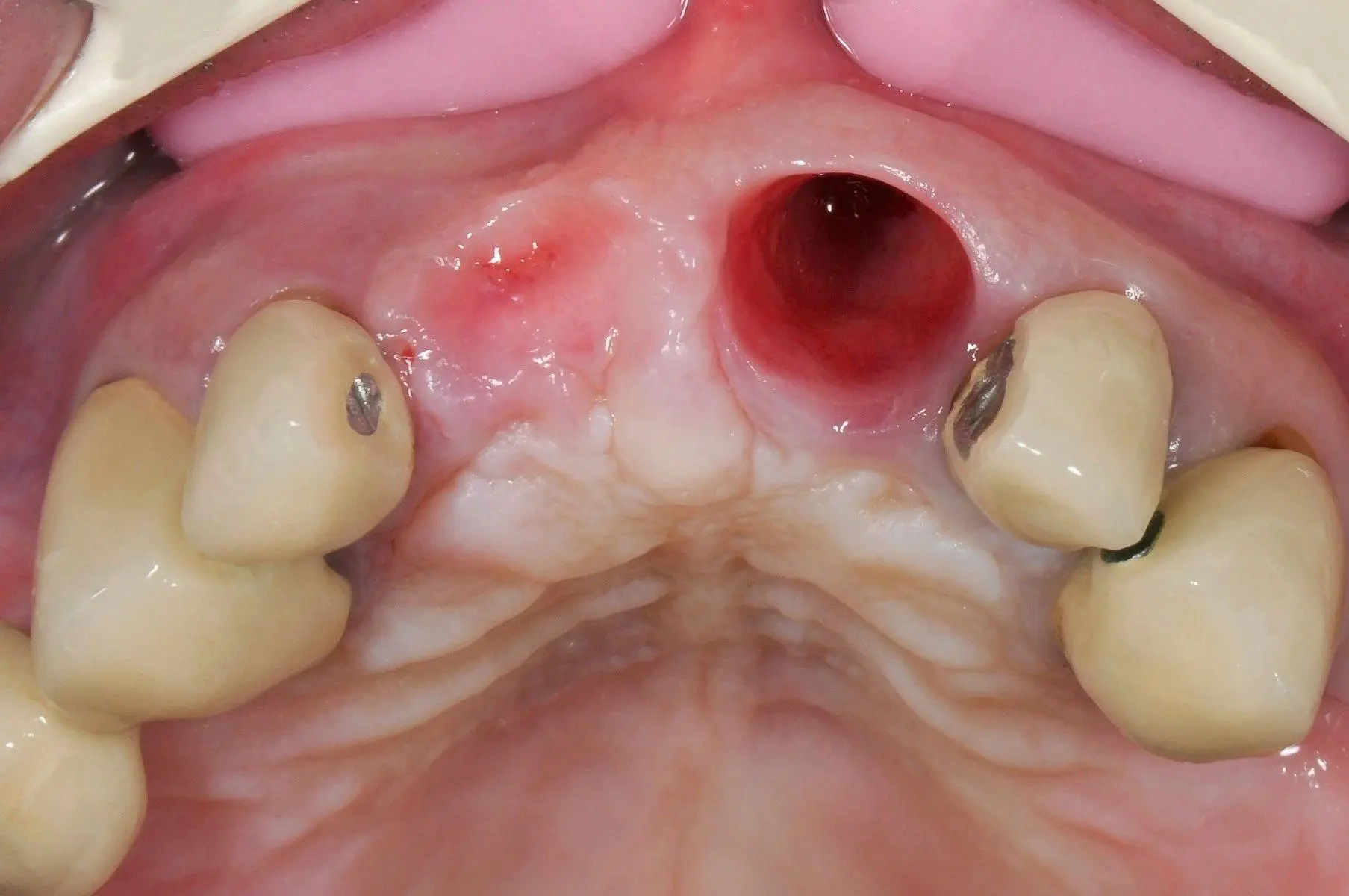
How Does Alveolitis Look? Structural Appearance
When you open your mouth wide and inspect the extraction site under a bright light with the help of a mirror, you can visually identify how does alveolitis look through these structural characteristics:
- A Normal Healing Socket: Displays a dark red, almost black, healthy blood clot layer completely filling the cavity, or a white-grey layer of new healing tissue (fibrin fibers) forming over it. Patients frequently mistake this white fibrin tissue for an infection, but it is actually a sign of healthy structural healing.
- An Alveolitis (Dry) Socket: When inspecting the extraction cavity, the inside appears completely empty, like a dry well. The protective blood clot is entirely gone. At the base and along the lateral walls of the socket, bare, dry jawbone walls with a greyish, dull white, or yellowish tint are directly visible. Sometimes, the interior of the socket presents a greyish appearance due to decaying food debris.
How is Contemporary Alveolitis Treatment Done and How Does It Heal?
The definitive medical answer to the panicky query how to treat alveolitis is as follows: Alveolitis cannot be cured at home using hearsay methods, rubbing alcohol on the wound, or packing it uncontrollably with raw clove oil; immediate, professional intervention by a dentist is absolutely required.
The contemporary alveolitis treatment protocol applied by our oral and maxillofacial surgeons consists of these painless and comfortable steps:
1. Local Anesthesia and Socket Lavage
To completely neutralize the intense tenderness felt when the patient sits in the chair, a mild local anesthesia is administered first. Following this, the degenerated clot remnants and decaying food debris accumulated inside the socket are gently flushed out (irrigated) using sterile saline or 0.12% chlorhexidine solutions at room temperature. To avoid exposing more bare bone surfaces, scraping the socket walls (curettage) is strictly discouraged in contemporary clinical guidelines.
2. Medical Dressing and Advanced Therapeutic Paste Application
To fully insulate the exposed, sensitive bone nerve endings from the oral environment and stop the pain within seconds, a specialized medicated dressing is placed into the dry socket. The material preferred in our clinics is a therapeutic paste (such as alvogyl) which contains iodoform for antisepsis, carrier fibers, and a derivative of clove oil (eugenol) acting as a potent natural analgesic. The moment this material is placed into the cavity, it blankets the bare bone surfaces like a cap and stops the throbbing pain instantly. Because these smart pastes possess a self-resorbing structure, they do not require subsequent surgical removal; they dissolve slowly beneath the tissues and are naturally shed.
3. Advanced Technologies: Laser Photobiomodulation
In modern dentistry, Low-Level Laser Therapy (LLLT) and photobiomodulation technologies are implemented for recalcitrant alveolitis cases that do not respond to traditional dressings. Diode laser beams at a wavelength of 660 nm are applied inside the dry socket for a few minutes. The laser stimulates local blood flow by upgrading mitochondrial ATP production within the cells, rapidly suppressing local inflammation and accelerating the formation of new granulation tissue to cover the exposed bone matrix.
Frequently Asked Questions
Does alveolitis resolve on its own?
Yes. Alveolitis is a self-limiting condition. Even without treatment, new tissue (granulation tissue) rising from the underlying jawbone gradually covers the exposed bone within an average of 2 to 3 weeks, resolving the issue.
What happens if alveolitis is left untreated?
First, you experience severe, chronic pain that lasts for weeks, severely impairs your quality of life, and does not respond to standard painkillers. The second stage occurs when bacteria from the oral cavity penetrate deep into the exposed jawbone, causing the infection to spread into the bone itself. This can lead to inflammation of the jawbone and irreversible necrosis (bone death) of the surrounding bone tissue, potentially necessitating major surgical interventions.
How long does it take for alveolitis to heal?
Following a medical dressing applied by a physician, the severe, throbbing pain subsides by 80–90% and comes under control within the first 24 to 48 hours. However, it takes an average of 7 to 10 days for the extraction socket to fill biologically with new tissue, for the bone to be fully covered by soft tissue, and for the wound to close completely.
Is it necessary to use antibiotics to treat alveolitis?
No, it is not. One of the most common clinical errors is immediately prescribing systemic antibiotics to a patient upon diagnosing alveolitis. In routine cases, the use of antibiotics contributes nothing to the speed of recovery. Antibiotics are indicated only and exclusively when it is preferred if the patient has a systemic immune deficiency, such as uncontrolled diabetes, or if the alveolitis is accompanied by signs of systemic infection such as facial swelling, high fever, excessive lymph node enlargement, and purulent discharge.
About the Author








