

What Is Tooth Root Cyst? Symptoms, Root Canal & Surgery
Don't put off your smile. Message us now to discuss your treatment options with our expert dentists.
WhatsAppSystemic oral configuration stands as one of the primary mechanisms protecting the overall biological balance of the human body. While dental decay or structural fractures forming along the visible crown surfaces are easily detected and treated, specific pathologies developing deep within the alveolar bone matrix around root structures progress in a highly silent and dangerous manner. The most prominent among these hidden pathologies is the tooth root cyst (known medically as a periapical cyst or radicular cyst). Tooth root cysts frequently develop without producing any physical pain or early symptoms, expanding silently within the jawbone for years while resorbing surrounding bone structures. If left unmanaged, this condition can weaken the jaw architecture, cause the loss of healthy adjacent teeth, and trigger facial facial asymmetry. This comprehensive YMYL guide covers the biological classification, advanced digital diagnostics, and modern treatment methodologies regarding root cyst pathologies.
Table of Content
- What is a Tooth Root Cyst and What Causes a Tooth Root Cyst?
- What Are the Prominent Tooth Root Cyst Symptoms?
- Why is an Upper Tooth Root Cyst More Dangerous?
- How to Treat a Tooth Root Cyst: Advanced Clinical Pathways
- How is Tooth Root Cyst Surgery Done?
- Essential Post-Operative Instructions After a Tooth Root Cyst Surgery
- Frequently Asked Questions
What is a Tooth Root Cyst and What Causes a Tooth Root Cyst?
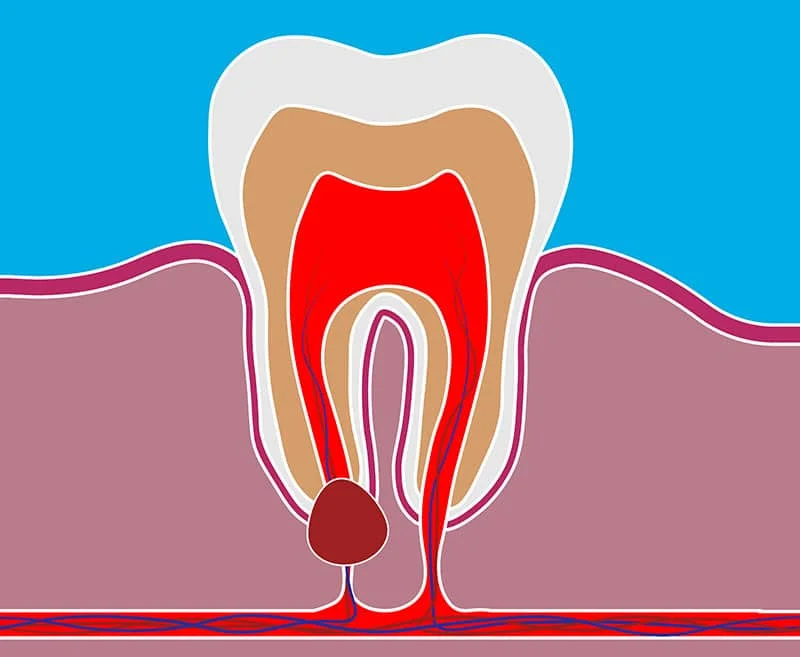
In clinical maxillofacial pathology, the definitive answer to what is a tooth root cyst is this: It is an inflammatory, fluid-filled or semi-solid fluid sac lined with an epithelial layer, forming at the root apex of a non-vital (dead) tooth as a chronic biological response to ongoing bacterial infection.
But, exploring the cellular mechanisms behind it, what causes a tooth root cyst and what factors trigger these jaw bone lesions?
- Unmanaged Deep Dental Decay: If a surface cavity is left untreated over a long duration, bacteria aggressively migrate into the internal pulp chamber. This triggers irreversible inflammation, cutting off vascular supply and causing nerve death (pulpa necrosis). Bacteria and toxic cellular byproducts track down the root canals, exiting the root apex into the surrounding bone.
- Failing Historical Root Canal Therapies: If a previous endodontic treatment failed to thoroughly disinfect the micro-canal matrix, or if the root canal fill failed to achieve a dense, micro-leakage-proof apical seal, stagnant bacteria will re-activate, triggering a tooth root cyst root canal reinfection framework.
- Physical Dental Trauma: A sudden high-velocity impact to a tooth (from sports injuries or accidents) can sever the vital neurovascular packet entering the root apex, even if the outer crown remains unbroken. The pulp tissue undergoes silent necrosis, eventually transforming into an apical cyst.
- Impacted Crown Follicles: The developmental sac wrapping around an impacted wisdom tooth or impacted canine can undergo structural changes over time, developing into distinct odontogenic cysts (such as dentigerous cysts) that resorb surrounding bone.
What Are the Prominent Tooth Root Cyst Symptoms?
The most dangerous aspect of periapical cysts is that during their early and intermediate developmental stages, they are entirely asymptomatic (painless). Most patients only discover they have a bone lesion during routine dental visits when a digital panoramic x-ray reveals the pathology. However, as the fluid volume increases or enters an acute inflammatory phase, distinct tooth root cyst symptoms begin to show:
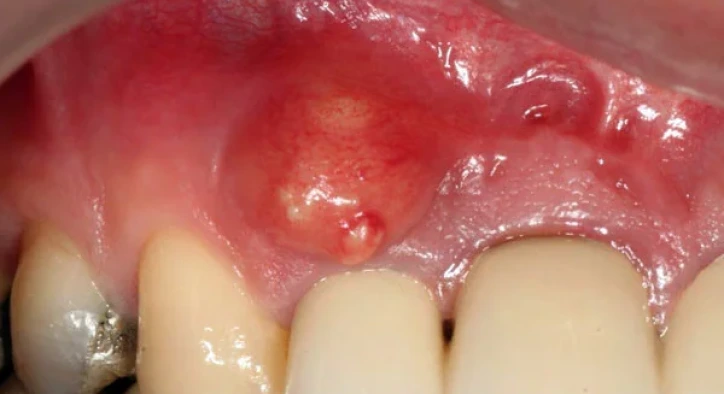
- Gingival Fistulas and Localized Swelling: As internal fluid pressure builds, the infection resorbs a path through the hard cortical jawbone toward the soft tissues. A small pimple-like drainage tract (fistula) forms on the gums, periodically discharging pus and causing a foul taste or bad breath.
- Dull Pain During Mastication or Pressure: While the tooth may remain painless under standard resting conditions, applying physical pressure, biting hard foods, or tapping the tooth triggers a deep, dull ache inside the bone due to the underlying cyst capsule.
- Facial Asymmetry and Firm Swellings: Once the lesion expands beyond the structural bone boundaries, it thins the outer cortical plate, producing a firm, noticeable protrusion under the cheek, jawline, or palate.
- Mobility and Migration of Adjacent Teeth: As the cyst expands, it resorbs the critical alveolar bone holding neighboring teeth in position. Lacking bony support, pristine adjacent teeth can begin to loosen, tilt, or shift out of alignment.
- Dark Grey or Matte Tooth Discoloration: Because the source tooth has lost its blood supply and underwent necrosis, the enamel loses its natural translucency, transforming into a dull, dark grey or matte black color.
Why is an Upper Tooth Root Cyst More Dangerous?

While bone cysts can develop in any area of the jaws, an upper tooth root cyst presents distinct anatomical risks due to its proximity to the maxillary sinus cavities.
The roots of the upper premolars and molars sit directly beneath the thin floor of the sinus cavities. When a cyst forms at the apex of these upper teeth, it tracks upward, resorbing the thin bony sinus floor and expanding into the open sinus space. This triggers chronic odontogenic maxillillary sinusitis, presenting as persistent one-sided nasal congestion, thick post-nasal drip, foul nasal odors, and deep facial pressure headaches beneath the eyes. Managing this advanced setup requires a complex combined oral and ENT surgical approach.
How to Treat a Tooth Root Cyst: Advanced Clinical Pathways
When exploring how to treat a tooth root cyst or how to heal a tooth root cyst, it is critical to state an absolute clinical fact: Tooth root cysts can never be resolved at home using natural remedies, herbal flushes, or over-the-counter antibiotics. Antibiotics can temporarily suppress acute swelling by lowering local bacterial activity, but as long as the structural epithelial cyst bag remains intact inside the bone, the lesion will resume growing the moment the medication course ends. Complete healing requires dedicated clinical intervention.
Advanced tooth root cyst treatment protocols follow two primary clinical pathways depending on the overall diameter of the lesion and the level of bone destruction:
1. Specialized Endodontic Therapy (Non-Surgical Approach)
If the periapical lesion is small (<5-7 mm) and bone tracking is minimal, a non-surgical tooth root cyst root canal intervention is highly effective. An endodontist opens the tooth to access the root canals, executing intensive debridement using specialized antiseptic flushes and advanced laser disinfection. A high-pH medical paste, such as calcium hydroxide, is packed into the canals and left for several weeks. This alters the local acidic environment of the cyst, neutralizing bacterial toxins, destroying epithelial cells, and prompting the surrounding bone to naturally regenerate. Once radiological tracking shows bone healing, the permanent root canal fill is completed.
2. Micro-Surgical Enucleation and Apicoectomy
If the cyst is too large to be cleared through the root canals, or if the tooth is covered by a premium zirconium or porcelain bridge that cannot be removed, a specialized tooth root cyst surgery is mandatory. This micro-surgical procedure is known as an apicoectomy (root-end resection) combined with cyst enucleation.
How is Tooth Root Cyst Surgery Done?
Conducted by an expert oral and maxillofacial surgeon inside a fully sterile surgical suite, the sequence of how tooth root cyst surgery is done follows these precise milestones:
- Targeted Local Anesthesia Block: Advanced local anesthetic configurations are delivered to the target quadrant, fully turning off pain receptors in the tooth and surrounding bone matrix to guarantee an entirely painless procedure.
- Tissue Flap Elevation: A small, controlled micro-incision is tracked along the gumline. The soft tissue flap is gently reflected to expose the underlying cortical bone surface covering the cyst.
- Creating a Bone Window and Enucleation: Utilizing specialized cooled surgical drills or advanced piezoelectric bone surgery inserts, a small window is micro-cut through the bone to access the lesion. The surgeon uses precision curettes to carefully separate the entire epithelial cyst sac from the surrounding bone matrix, extracting the capsule completely intact (enucleation) to prevent recurrence.
- Apicoectomy (Root-End Resection): The apical 3 mm of the infected tooth root is cleanly excised. Using specialized retro-grade preparation tips, a micro-cavity is prepped into the cut root surface from behind and sealed using advanced biocompatible bioceramic aggregates (MTA) to block future bacterial leakage.
- Bone Greft (Bone Powder) Integration: If extracting the large cyst sac leaves a significant structural defect inside the jawbone, high-grade bone powder (bone graft) materials are packed into the empty cavity to accelerate bone regeneration, covered with a protective bio-resorbable membrane.
- Flap Alignment and Suturing: The soft tissue flap is neatly realigned and secured using micro-sutures. The entire procedure takes between 30 and 60 minutes, depending on the structural volume of the cyst.
Tailoring the Treatment Plan
Maxillofacial specialists utilize this precise matrix to match the cyst profile with the optimal clinical intervention:
|
Cyst Diameter & Bone Profile |
Primary Selected Treatment |
Advanced Material Requirements |
|
Small Apical Lesions (< 5 mm) |
Advanced Non-Surgical Endodontics |
Calcium hydroxide packing; zero bone graft required. |
|
Medium Cyst, Unresponsive to Root Canals |
Surgical Apicoectomy & Enucleation |
Precision micro-endodontic retro-sealing with MTA. |
|
Large Cyst, Thinning the Jaw Architecture |
Full Enucleation Surgery + Grafting |
Dense bone powder packing and resorbable membrane lock. |
|
Extensive Cyst Causing Vertical Root Fracture |
Tooth Extraction & Complete Curettage |
Removal of the unsalvageable root followed by delayed implant placement. |
Essential Post-Operative Instructions After a Tooth Root Cyst Surgery
The ultimate rate of bone regeneration and tissue healing depends directly on how meticulously the patient follows these tooth root cyst post-operative instructions during the initial week:
- Consistent Ice Pack Application: Apply an external ice pack wrapped in a cloth against your cheek over the surgical zone for 10-minute intervals during the first 24 hours. This restricts local capillary dilation, minimizing facial swelling and post-surgical edema.
- Do Not Spat or Rinse on Day One: Swallowing your saliva and minor blood traces normally is mandatory on the initial day. Spitting or aggressive mouth rinsing creates negative oral pressure that can dislodge the blood clot, tearing the micro-sutures and bleeding the bone defect.
- Dietary Modifications: For the first 3 days, strictly avoid hard, crunchy, heavily spiced, hot, or granular foods (such as chips, rice, or seeds) that can lodge beneath the flap. Maintain a lukewarm soft diet composed of purees, smooth soups, and yogurt, always chewing on the unoperated side.
- Meticulous Oral Hygiene Execution: Do not brush directly against the suture line on the first day. Adjacent quadrants must be brushed normally. Starting on day two, implement a specialized ultra-soft post-surgical brush to gently clean the area. Prescribed antiseptic mouthwashes should be introduced on day two, held gently over the area without aggressive swishing.
- Strict Smoking and Alcohol Prohibitions: Nicotine heavily constricts local blood vessels, reducing oxygen delivery to the healing bone matrix. This can cause suture breakdown, graft contamination, and failed bone healing. Smoking must be strictly paused for at least 1 full week post-surgery.
Frequently Asked Questions
Will I experience intense pain during or after a tooth root cyst surgery?
Because the surgical phase is completely managed under advanced local anesthetic blocks, it is impossible to feel any sharp pain or distress during the procedure. Once the numbness wears off hours later, a mild-to-moderate dull ache and localized tenderness are natural biological responses to bone modification. This discomfort is completely controlled using the standard anti-inflammatory painkillers prescribed by your surgeon.
When are the surgical sutures removed and how long is the healing timeline?
The soft tissue sutures are checked and painlessly removed by your specialist inside the clinic exactly 7 to 10 days post-surgery. While the outer soft tissue flap stabilizes within 2 weeks, the internal bone remodeling process required to fully fill the empty bone defect with dense natural bone takes between 3 and 6 months.
Can an untreated tooth root cyst transform into a malignant tumor or cancer?
Radicular and periapical cysts are entirely benign patholojik formations, meaning they do not possess a biological tendency to transform into cancer. However, if left untreated, they will continue to expand indefinitely, which can lead to spontaneous jaw fractures (pathological fractures), permanent lip numbness from nerve compression, and severe bone infections (osteomyelitis). Therefore, prompt clinical removal is necessary regardless of their benign classification.
About the Author